management of vertebral compression fracture
- related: MSK
- tags: #msk
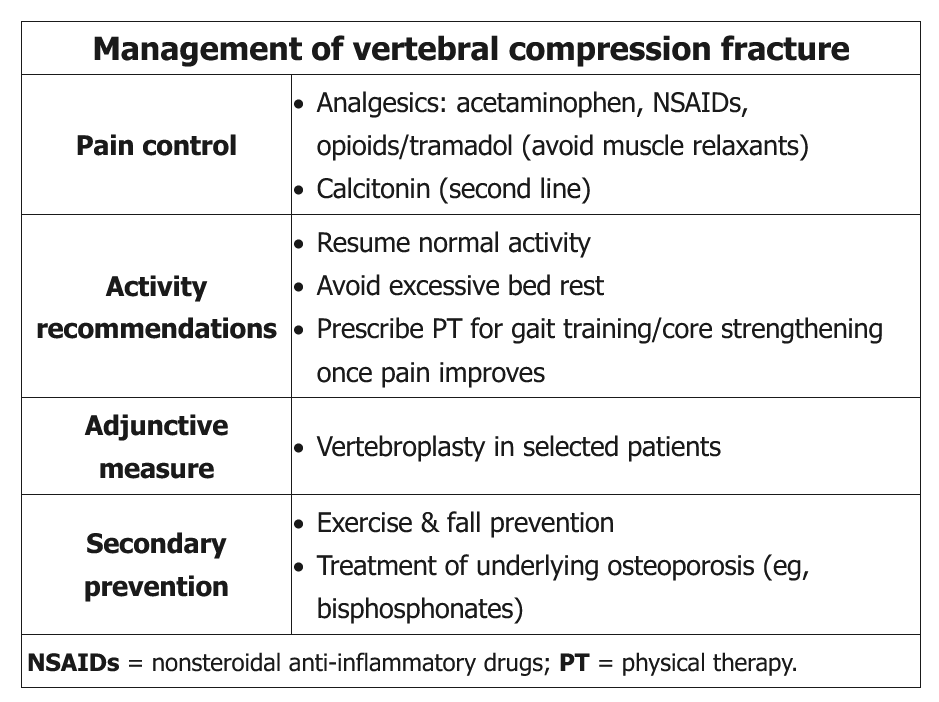
This patient has acute back pain and vertebral tenderness after a ground-level fall. X-ray confirms a vertebral compression fracture (VCF), likely due to postmenopausal osteoporosis. Initial management of pain following VCF may require simple analgesics (eg, acetaminophen, nonsteroidal anti-inflammatory drugs), opioid analgesics, or, occasionally, inpatient hospitalization for parenteral opioids. If pain persists, calcitonin nasal spray can provide additional pain relief. However, skeletal muscle relaxants are not generally recommended due to adverse effects that are magnified in the elderly population (eg, drowsiness).
Patients with VCF should be encouraged to ambulate and resume normal activity as soon as possible. After the pain is controlled and the patient is ambulating adequately, a dedicated course of physical therapy to address core strengthening and gait training for fall prevention can be implemented. Secondary preventive measures include exercise (eg, flexibility and balance exercises, resistance training), management of the underlying osteoporosis (eg, bisphosphonates, calcium, vitamin D), and avoidance of lifestyle risk factors (eg, smoking).
Unnecessary bed rest is associated with decreased functional capacity and additional loss of bone density and is not recommended.
Pain from acute VCF usually improves within 4-6 weeks. Patients with refractory pain lasting >6 weeks can be considered for vertebral augmentation (eg, vertebroplasty, kyphoplasty), but these procedures are not recommended acutely.
Rigid thoracolumbar braces are not well-studied for VCF. Limited evidence suggests that they are not significantly better than soft braces or no bracing.